Losing functional vision in one eye—known as monocular vision—can drastically alter how you interact with the world. The shift from binocular to monocular vision problems disrupts depth perception, shrinks your field of view, and increases mental effort during routine tasks. Whether caused by stroke, trauma, or disease, this condition affects millions, yet remains widely misunderstood. The core challenges—impaired spatial judgment, visual fatigue, and heightened risk to the remaining eye—require more than medical treatment: they demand adaptation, protection, and long-term management. While the journey is often difficult, most people successfully regain independence by understanding the causes, mastering compensatory strategies, and safeguarding their sole functioning eye. This guide explores the medical origins of monocular vision loss, how to diagnose it accurately, practical ways to adapt, and essential steps to protect your remaining sight.
Common Visual Challenges with Monocular Vision
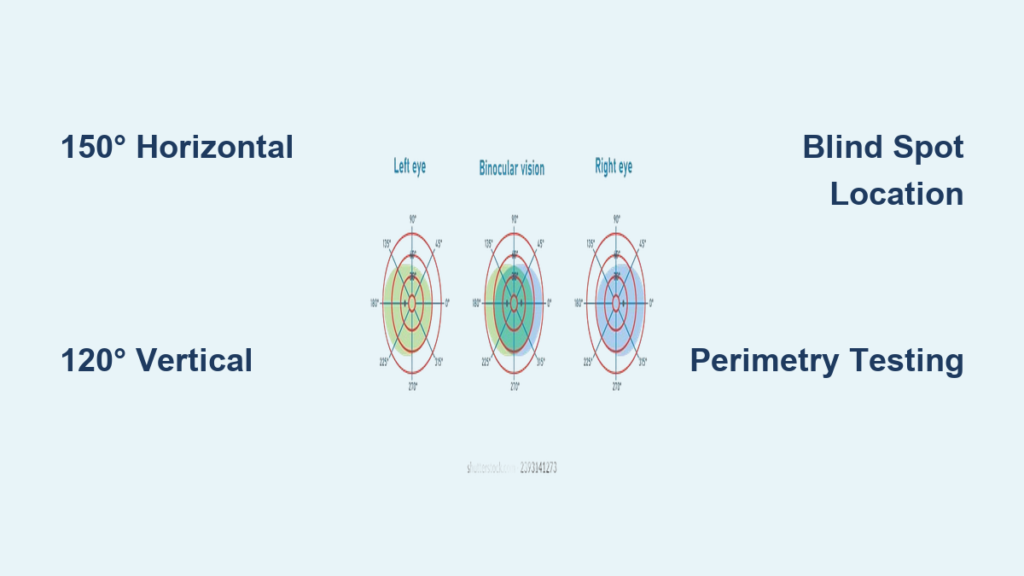
Reduced Peripheral Awareness on the Affected Side
With only one eye, your horizontal field of view drops by about 30% on the side of vision loss, narrowing from a typical 180° to roughly 140°. This creates a blind spot that makes it easy to miss objects, trip on obstacles, or misjudge traffic when crossing streets. You might bump into doorframes, overlook items on a table, or feel disoriented in crowded spaces.
To compensate:
– Turn your head fully toward the side of vision loss before moving.
– Use wide-angle mirrors in your car or home.
– Develop a habit of scanning your environment before walking or driving.
Without active head movement, navigation becomes risky—especially in low light or busy areas.
Depth Perception Difficulties Without Stereoscopic Vision
The most immediate monocular vision problem is the loss of 3D depth perception. Binocular vision allows your brain to calculate distance using slight differences between what each eye sees. With one eye, this stereoscopic cue vanishes.
Tasks become harder, such as:
– Judging step height
– Pouring liquids without spilling
– Reaching accurately for objects
– Parking a car or threading a needle
However, your brain can learn to rely on monocular depth cues:
– Motion parallax (closer objects move faster across your vision)
– Relative size (familiar objects appear smaller when farther away)
– Shadows and lighting gradients
– Texture density (e.g., grass looks finer with distance)
Practice improves accuracy, but expect initial misjudgments—they’re normal.
Increased Visual Fatigue and Cognitive Strain
Using one eye forces your brain to work harder to interpret space and movement. This leads to visual fatigue, especially during:
– Long reading sessions
– Driving in complex traffic
– Walking on uneven terrain
Symptoms include:
– Headaches
– Eye strain
– Mental exhaustion
– Slower reaction times
While fatigue doesn’t damage your eye, it can compromise safety and performance. Combat it by:
– Taking frequent visual breaks
– Using bright, even lighting
– Wearing up-to-date corrective lenses
– Avoiding cluttered or visually overwhelming environments
Key Medical Causes of Monocular Vision Loss
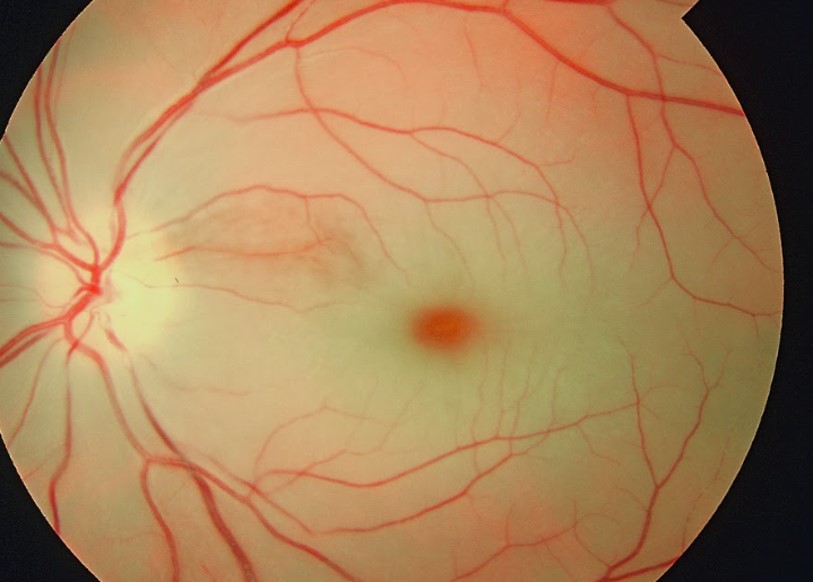
Central Retinal Artery Occlusion (CRAO)
Sudden, Painless Vision Loss with Cherry-Red Spot
A central retinal artery occlusion (CRAO) causes immediate, painless blindness in one eye. The retina turns white due to lack of blood flow, except at the macula, where a cherry-red spot appears. This is a medical emergency—treatment within 90 minutes may restore some vision.
Branch retinal artery occlusion (BRAO) affects only part of the visual field and may mimic a stroke.
Common causes:
– Emboli from carotid artery disease
– Atrial fibrillation
– Vasculitis or clotting disorders
Even if vision doesn’t return, identifying the cause helps prevent stroke.
Optic Neuritis: Inflammation Linked to Multiple Sclerosis
Pain When Moving the Eye
Optic neuritis involves inflammation of the optic nerve, often tied to multiple sclerosis. Symptoms develop over days and include:
– Blurred or dimmed vision
– Washed-out colors
– Central blind spot
– Pain when moving the eye
MRI typically shows nerve swelling and enhancement. Most people regain good vision, but subtle depth and contrast issues may remain.
Blood tests and imaging rule out mimics like neuromyelitis optica (NMO), which causes more severe, often bilateral damage.
Non-Arteritic Ischemic Optic Neuropathy (NAION)
Sudden Vision Loss Without Pain
NAION is the most common optic nerve cause in adults over 50. It leads to:
– Sudden vision loss, often upon waking
– Altitudinal field defect (loss in top or bottom half)
– Swollen optic disc
– No eye pain
Risk factors include:
– Sleep apnea
– Diabetes
– High blood pressure
– Use of erectile dysfunction drugs (e.g., sildenafil)
Recovery is limited. The other eye often has a “crowded disc,” increasing its risk—so monitoring is essential.
Giant Cell Arteritis (Arteritic AION): A Vision Emergency
Immediate Steroids Required
Arteritic AION, caused by giant cell arteritis (GCA), is a vision-threatening emergency in people over 60. Symptoms include:
– Vision loss (usually painless)
– Headache, scalp tenderness, jaw pain when chewing
– High ESR and CRP levels
– Chalky-white, swollen optic disc
Start high-dose steroids immediately—even before biopsy confirms GCA. Delay risks blindness in both eyes.
Temporal artery biopsy is the diagnostic gold standard.
Retinal Detachment and Macular Disorders
Flashing Lights and a “Curtain” Over Vision
Sudden floaters, flashes, or a dark curtain over your vision signal retinal detachment—a surgical emergency. Repair within days can save vision.
Other macular causes:
– Central serous retinopathy: Fluid under the macula causes distorted vision
– Diabetic macular edema: Swelling from blood vessel leaks
– Cystoid macular edema: Fluid buildup after surgery or inflammation
OCT imaging detects subtle changes not visible on exam.
How Doctors Diagnose Monocular Vision Problems
Critical Clues from Your Medical History
Your symptoms point to specific causes:
– Wavy vision → macular disease
– Flashing lights → retinal detachment
– Faded colors → optic nerve issue
– Eye pain with movement → optic neuritis
– Jaw pain when chewing → giant cell arteritis
Always report:
– Onset speed (sudden vs. gradual)
– Neurological symptoms (numbness, weakness)
– Medications (e.g., Viagra, blood thinners)
– Medical conditions (diabetes, MS, lupus)
Swinging Flashlight Test for Optic Nerve Damage
The swinging flashlight test detects a relative afferent pupillary defect (RAPD)—a key sign of optic nerve or severe retinal damage.
How it works:
– Light is swung between eyes.
– In healthy vision, pupils constrict equally.
– In monocular nerve damage, pupils dilate when light hits the bad eye.
An RAPD confirms real disease. Its absence suggests functional (non-organic) vision loss.
Imaging and Lab Tests to Pinpoint the Cause
OCT and MRI Scans
- OCT measures retinal layers and detects:
- Macular edema
- Nerve fiber thinning (in optic atrophy)
-
Vitreomacular traction
-
MRI with contrast rules out:
- Optic neuritis (enhancing nerve)
- Tumors
- MS lesions
Blood Tests and Biopsy
Essential for systemic causes:
– ESR and CRP: Elevated in giant cell arteritis
– NMO-IgG antibody: Diagnoses neuromyelitis optica
– Syphilis, Lyme, HIV tests: If infection suspected
– Genetic testing: For Leber hereditary optic neuropathy (LHON)
Temporal artery biopsy confirms GCA but should not delay steroid treatment.
Practical Adaptation Techniques for Daily Life
Reaching, Pouring, and Moving Safely
Simple changes reduce accidents:
– Pouring liquids: Rest the container’s lip on the cup before pouring.
– Reaching for objects: Use an open hand and move slowly—confirm contact by touch.
– Using stairs: Feel each step with your foot before stepping down.
– Cooking: Keep pot handles turned inward and avoid carrying hot liquids.
Practice builds confidence and reduces spills or burns.
Making Your Home Safer
- Keep floors clear of clutter
- Use non-slip mats in bathrooms
- Install grab bars and handrails
- Use bright, even lighting—avoid shadows
- Add contrast strips on stair edges
Training Your Brain to Judge Depth
Rebuild spatial confidence with practice:
– Catch and throw a ball
– Reach for objects at different distances
– Walk through obstacle courses slowly
– Use touch to confirm distance
Over time, your brain learns to use motion and size cues more effectively.
Driving with One Eye: Rules and Safety Tips

Legal Requirements in the U.S. and Beyond
You can legally drive in all 50 U.S. states with monocular vision if:
– Your remaining eye meets acuity and field standards
– You have a doctor’s certification
– You notify your licensing agency (if required)
Wait at least 3 months after vision loss to adapt before driving.
Safe Driving Habits
- Turn your head more, especially toward the blind side.
- Use extended or convex side mirrors.
- Rely on backup cameras and blind-spot monitors.
- Avoid night driving if glare or depth issues persist.
Consider a driving rehabilitation program for monocular drivers.
Protecting Your Remaining Eye: A Lifelong Priority

Preventing Injury with Safety Eyewear
Since you depend on one eye, protection is non-negotiable:
– Wear polycarbonate safety glasses during:
– DIY projects
– Gardening
– Sports (especially ball or racquet games)
– Any task with flying debris
Avoid metal-on-metal work (e.g., hammering), which can create eye-penetrating shrapnel.
Routine Eye Exams Are Essential
Schedule annual checkups to monitor for:
– Glaucoma
– Cataracts
– Macular degeneration
Update your glasses prescription for both distance and near vision. Even small refractive errors increase strain.
Planning Surgery on Your Good Eye
If you need cataract or other eye surgery:
– Understand all risks and recovery time
– Arrange for post-op care—you may be patched
– Avoid day surgery discharge if going home alone with a patch
– Inform your surgeon of your monocular status
Never undergo elective surgery without a clear recovery plan.
When to Patch the Poor Eye for Clarity
If your weaker eye causes blurred vision, double images, or confusion, occlusion therapy helps.
Options include:
– Eye patch (temporary use)
– Frosted lens in glasses
– Opaque contact lens (rare)
Patching reduces brain conflict and improves clarity. Use during:
– Early adaptation phase
– Visually demanding tasks
– Monocular diplopia (double vision in one eye)
Support and Long-Term Outlook
Can You Register as Visually Impaired?
Most countries do not classify monocular vision as legal blindness. Registration usually requires bilateral vision loss.
However, you may still access:
– Low vision clinics
– Driving rehabilitation programs
– Workplace accommodations
A consultant ophthalmologist determines eligibility.
Key Support Resources
- RNIB (Royal National Institute of Blind People): Advice, tools, and emotional support
- SeeAbility: Support for those with learning disabilities and vision loss
- Online forums: Connect with others facing similar challenges
Emotional adjustment takes time—support groups help.
Prognosis and Recovery: What to Expect
Recovery Varies by Cause
- Optic neuritis: 80–90% regain 20/40 vision or better
- NAION: Limited recovery; focus on protecting the other eye
- CRAO: Only 30–35% regain some vision
- LHON: Spontaneous recovery possible, especially with T14484C mutation
Even without vision return, most people adapt well to daily life.
Prevent Future Vision Loss
Focus on systemic health:
– Control blood pressure, diabetes, cholesterol
– Take aspirin or statins if indicated
– Quit smoking
– Treat sleep apnea
– Monitor carotid artery health
Preventing stroke and vascular events protects both eyes—and your brain.
Final Note: Monocular vision problems are challenging but manageable. With the right diagnosis, adaptation strategies, and protective habits, most people live full, independent lives. Early action, regular eye care, and lifestyle adjustments are the pillars of long-term success.