Peering into a drop of blood under the microscope reveals a dynamic world of millions of tiny, disc-shaped cells gliding through plasma—each one a vital courier of oxygen. When viewed at 1000x magnification with oil immersion, red blood cells (RBCs) display a striking uniformity: round, pinkish discs with a pale center, moving like coins in a fluid stream. These anucleate, biconcave cells, measuring 6–8 µm in diameter, make up 40–45% of blood volume and are the workhorses of gas exchange. Their unique shape—thicker at the edges and indented in the center—creates central pallor, occupying about one-third of the cell’s width, a hallmark of healthy erythrocytes. But beyond their standard appearance lies a diagnostic treasure trove: changes in size, color, shape, or arrangement can signal everything from iron deficiency to life-threatening hemolytic disorders. Whether stained with Wright’s, Giemsa, or H&E, RBC morphology offers a real-time window into systemic health. This guide explores how to identify normal and abnormal red blood cells under the microscope, interpret staining patterns, avoid common artifacts, and understand the clinical meaning behind what you see—all grounded in current hematological science.
How to Identify Normal Red Blood Cells Under the Microscope
Biconcave Shape and Central Pallor
The defining feature of a healthy red blood cell is its biconcave disc shape, which appears under the microscope as a round cell with a pale central area—the central pallor. This structural design maximizes surface area for efficient oxygen and carbon dioxide exchange while allowing RBCs to deform and squeeze through narrow capillaries as small as 3 µm. In a well-prepared peripheral blood smear, normal RBCs are evenly distributed, non-overlapping, and maintain a consistent size. The central pallor should occupy roughly one-third of the cell’s diameter; if it’s larger, the cell may be hypochromic (low hemoglobin), a clue to iron deficiency. At 100x oil immersion, this depression is clearly visible, especially with Wright’s stain, which highlights hemoglobin-rich areas in pink.
Uniform Size, Color, and Distribution
Normal RBCs are normocytic (6–8 µm) and normochromic (adequately hemoglobinized). They appear pink to light blue-pink with Wright’s stain, red-orange with Giemsa, and bright red in H&E-stained tissue sections. Mature RBCs lack a nucleus, distinguishing them from nucleated red cell precursors seen in bone marrow or pathological conditions like severe anemia. Their smooth, regular borders contrast sharply with abnormal forms such as echinocytes or schistocytes. Any variation in size (anisocytosis) or shape (poikilocytosis) warrants further investigation and may indicate underlying disease.
Abnormal RBC Shapes and Their Clinical Significance
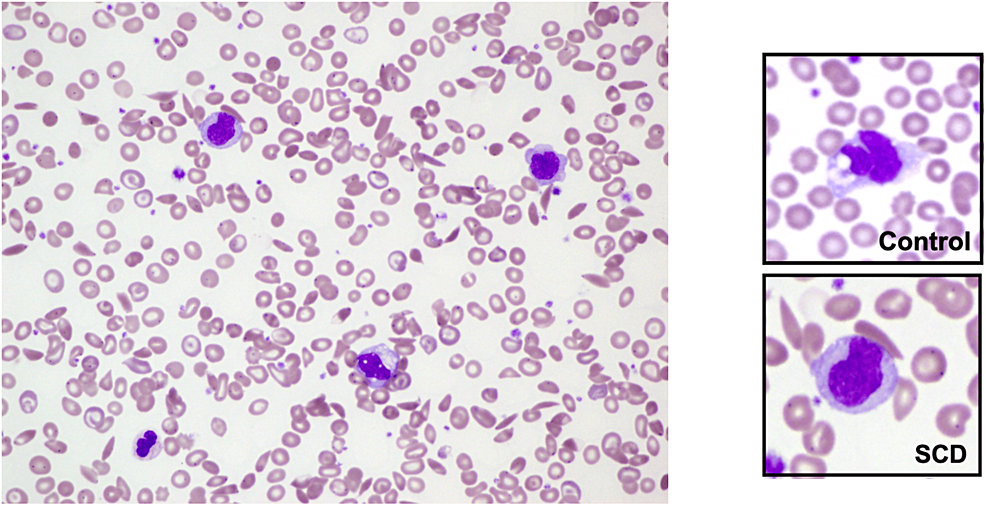
Sickle Cells in Sickle Cell Disease
Sickle cells (drepanocytes) are crescent- or sickle-shaped RBCs caused by the HbS mutation. These rigid, pointed cells form under low-oxygen conditions and can obstruct microcirculation, leading to vaso-occlusive crises. They are best seen on peripheral smears stained with Wright’s stain and appear alongside other findings like target cells or Howell-Jolly bodies. Their presence is diagnostic when combined with clinical symptoms such as chronic hemolytic anemia, pain episodes, and organ damage.
Spherocytes in Hemolytic Anemia
Spherocytes are small, round RBCs with no central pallor, appearing densely stained and darker than normal cells. They result from partial membrane loss, commonly in hereditary spherocytosis or autoimmune hemolytic anemia (AIHA). Due to reduced deformability, they are trapped and destroyed in the spleen. Identifying spherocytes prompts further testing, such as the Coombs test or osmotic fragility test, to confirm diagnosis.
Target Cells in Liver and Hemoglobin Disorders
Target cells (codocytes) exhibit a bullseye appearance: a central hemoglobin spot, a pale ring, and an outer hemoglobin rim. They are associated with liver disease, thalassemia, and other hemoglobinopathies. In thalassemia, excess alpha globin chains damage the membrane; in liver disease, altered lipid metabolism affects membrane fluidity. While not specific, their abundance supports further evaluation—especially if microcytosis is also present.
Schistocytes and Microangiopathic Hemolysis
Schistocytes—fragmented, helmet-shaped RBCs—are key indicators of microangiopathic hemolytic anemia (MAHA). Seen in thrombotic thrombocytopenic purpura (TTP), disseminated intravascular coagulation (DIC), or mechanical heart valves, they form when RBCs are sheared by fibrin strands in small vessels. Even 1% schistocytes on a smear demand urgent clinical workup. Unlike echinocytes, which have uniform spicules, schistocytes have jagged, irregular edges.
How Staining Techniques Change RBC Appearance

Wright’s Stain: The Gold Standard
Wright’s stain is the most widely used method for peripheral smear analysis. It combines eosin (pink) and methylene blue to differentiate blood components. RBCs stain pinkish-red, with clear central pallor and visible polychromasia—a bluish tint indicating immature reticulocytes. Poor staining—too acidic or alkaline—can distort results: acidic smears make RBCs overly pink, masking pallor; alkaline smears give them a gray-blue hue.
Giemsa Stain for Detecting Parasites
Giemsa stain is preferred for identifying intraerythrocytic parasites. RBCs appear pink to red, while Plasmodium (malaria) shows purple nuclei and blue cytoplasm. Diagnostic features include ring forms and crescent-shaped gametocytes in P. falciparum. Babesia appears as paired pyriform bodies or Maltese cross tetrads—distinct from malaria. Caution is needed: staining artifacts can mimic parasites, so observing binary fission helps confirm Babesia.
H&E and Methylene Blue in Special Contexts
While H&E is used in tissue biopsies, it shows RBCs as bright red discs in vascular spaces—useful for detecting hemorrhage or vascular invasion. Methylene blue, though not used to stain mature RBCs, helps identify reticulocytes via supravital staining, where residual RNA binds the dye, giving cells a bluish-gray (polychromatophilic) appearance.
Common Artifacts That Mimic Disease
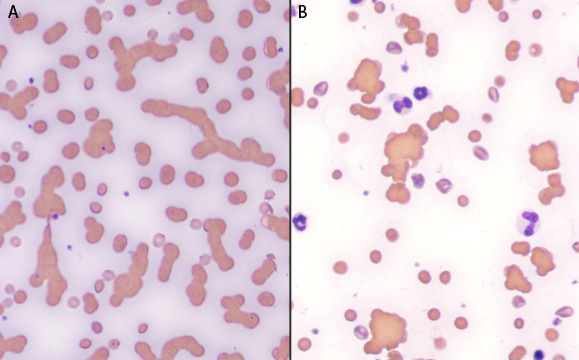
Rouleaux vs. True Agglutination
Rouleaux—RBCs stacked like coins—can mimic pathology but often result from high plasma proteins (e.g., multiple myeloma) or slide drying artifacts. Unlike cold agglutinin disease (where cells clump due to antibodies), rouleaux disperse in saline. They’re most common in the thick tail of the smear; always examine the monolayer for accurate assessment.
Echinocytes vs. Acanthocytes
Both have spiky projections, but echinocytes (burr cells) have small, uniform, evenly spaced spicules and may be reversible—seen in uremia, alcoholism, or drying artifact. Acanthocytes (spur cells) have irregular, thorny, asymmetric projections and indicate liver disease or abetalipoproteinemia. Context is key: echinocytes in a dehydrated sample may resolve with rehydration; acanthocytes persist.
Osmotic and Drying Artifacts
Poor technique causes misleading appearances. Hypotonic solutions (e.g., water contamination) cause swelling and lysis, leaving ghost cells—pale, ring-like remnants. Hypertonic conditions (high salt) cause crenation—shrunken, spiky cells resembling echinocytes. Always use isotonic diluents and fresh, properly anticoagulated blood to avoid false diagnoses.
Environmental Effects on Red Blood Cell Morphology
Hypotonic Lysis and Ghost Cells
In hypotonic environments, water enters RBCs via osmosis, causing them to swell and burst—hemolysis. Under the microscope, this appears as ruptured cells or ghost cells: pale, circular outlines with no hemoglobin. This is why IV fluids must be isotonic (e.g., 0.9% saline). In labs, accidental water contact during staining can create this artifact.
Hypertonic Crenation and Shrinkage
In hypertonic conditions (e.g., dehydration, high glucose), water leaves RBCs, causing crenation—a scalloped or spiky appearance. This is seen in diabetic ketoacidosis or poor sample handling. Unlike irreversible spherocytosis, crenated cells can regain normal shape when returned to isotonic media.
Plasmolysis in High-Solute Environments
Plasmolysis refers to osmotic shrinkage in high-solute conditions, often used interchangeably with crenation. It highlights the RBC’s dynamic response to osmotic balance and underscores the importance of proper sample preparation.
Clinical Diagnosis Through RBC Morphology
Classifying Anemia by Cell Size
Microscopic RBC analysis helps classify anemia:
– Microcytic (<6 µm): Iron deficiency, thalassemia—look for hypochromia and target cells.
– Macrocytic (>8 µm): B12/folate deficiency, alcoholism, liver disease—oval macrocytes suggest megaloblastic anemia.
– Normocytic: Chronic disease, hemolysis, acute blood loss—use reticulocyte count to differentiate.
Detecting Hemolysis and Bone Marrow Response
Polychromasia—bluish-gray reticulocytes—indicates active bone marrow compensation. It’s prominent in hemolytic anemia or post-hemorrhage recovery. A reticulocyte count (using new methylene blue) quantifies this response. High counts confirm effective erythropoiesis; low counts suggest marrow failure.
Identifying Infections Inside Red Blood Cells
Pathogens like Plasmodium and Babesia invade RBCs:
– Malaria: Ring forms, trophozoites, gametocytes—P. falciparum may have multiple rings per cell.
– Babesiosis: Paired pyriforms or Maltese crosses—differentiate from malaria using morphology and patient history.
Always correlate findings with travel history, fever, and lab markers like LDH and haptoglobin.
Preparing a Blood Smear for Accurate Analysis
Step-by-Step Smear Technique
- Collect blood in EDTA tube or via fingerstick.
- Place a small drop near the slide’s edge.
- Use a spreader slide at 30–45°, draw back into the drop, then push forward smoothly.
- Air-dry completely.
- Fix with methanol for 1–2 minutes.
- Stain with Wright’s or Giemsa, rinse, and dry upright.
Avoid excessive pressure or slow spreading to prevent distortion.
Quality Control: Finding the Monolayer
The ideal area for analysis is the monolayer—where cells are single, evenly spaced, and not overlapping. Avoid the thick head or feathered tail, where artifacts dominate. A poor smear with bubbles or uneven thickness reduces diagnostic value.
The Future: Lab-Grown Red Blood Cells and Advanced Imaging

Immortalized Cell Lines Like BEL-A2
To address blood shortages, scientists are developing in vitro-produced RBCs (cRBCs). The BEL-A2 line, derived from adult CD34+ cells, can proliferate for over 5 months and differentiate into functional reticulocytes expressing adult hemoglobin (HbA). Unlike iPSC-derived RBCs (which often produce fetal Hb), BEL-A2 offers a clinically relevant product.
Scaling Up with Bioreactors
Producing one transfusion unit (~2 × 10¹² RBCs) requires over 1000 liters of culture—impractical in flasks. Bioreactor technology enables high-density, scalable growth, overcoming cost and sterility challenges.
Clinical Trials: RESTORE and Beyond
The RESTORE trial (UK) is the first human study using lab-grown RBCs. Early data suggest longer survival—possibly due to younger cell age. In Barcelona, the Banc de Sang i Teixits (BST) produces rare-phenotype RBCs for sickle cell patients, reducing alloimmunization risk.
Advanced Imaging: SEM and Digital Microscopy
Scanning electron microscopy (SEM) reveals 3D surface details—spherocytes as smooth spheres, acanthocytes with jagged projections. While not routine, it’s vital for research. Digital systems like the BeaverLab Darwin M2 enable telepathology, AI-assisted analysis, and global diagnostics.
Final Note: Microscopic examination of red blood cells is both a science and an art. From detecting the subtle signs of iron deficiency to spotting schistocytes in a critical coagulopathy, every detail informs diagnosis and treatment. Always interpret findings in clinical context—combine smear results with CBC data, patient history, and symptoms. With emerging technologies like lab-grown blood and AI-driven imaging, RBC microscopy continues to evolve, offering deeper insights into health and disease. Whether you’re a student, clinician, or researcher, mastering this skill opens a direct window into the body’s most essential carriers of life.