If you’ve ever wondered what Demodex mites look like under a microscope, you’re not alone. These microscopic parasites live on nearly all adults, hiding in hair follicles and sebaceous glands. While invisible to the naked eye, they become strikingly clear under magnification—especially at X100 oil immersion. Using simple techniques like skin scrapings or adhesive tape biopsies, clinicians can detect Demodex folliculorum and D. brevis, distinguish their features, and assess their role in skin conditions like rosacea and sebaceous hyperplasia.
This guide breaks down exactly what to expect when viewing Demodex under the microscope, including visual characteristics, detection methods, species differences, and clinical significance—all based on documented microscopic analysis.
Optimal Magnification for Detection

Use X100 Oil Immersion for Clarity
To clearly identify Demodex mites, X100 magnification with oil immersion is essential. At this level, key anatomical details—such as segmented legs, body proportions, and head structure—become visible. Lower magnifications (e.g., X40) are useful for scanning the slide and locating follicular material, but X100 provides definitive identification.
Oil immersion improves resolution by reducing light refraction, allowing finer structures to stand out against the background. Without it, the translucent mites may blend into debris or keratin fragments, leading to false negatives.
Why Fluorescein Enhances Visibility
Placing samples in fluorescein solution before covering with a coverslip significantly boosts contrast. The dye does not stain the mite directly but creates a darker background, making the pale, semi-transparent body of Demodex easier to see. This technique is especially helpful in live, motile specimens where movement confirms viability.
In clinical studies, fluorescein-assisted microscopy has been used consistently by trained observers (e.g., ophthalmologists), ensuring reliable detection while minimizing observer variability.
How to Collect Samples for Microscopy
Skin Scraping Technique
Gently scrape the affected area—commonly the nose, forehead, or eyelid—with a sterile scalpel blade. Collect the debris into a drop of saline or mineral oil on a glass slide. This method works best for superficial dwellers like D. folliculorum, which inhabit the upper hair follicle.
Apply moderate pressure to avoid bleeding but ensure enough follicular contents are lifted. Examine immediately to observe motility, a sign of live mites.
Cellophane Tape Biopsy Method
Press a piece of clear adhesive tape onto cleansed skin, then lift and place it directly onto a microscope slide. This non-invasive method captures mites, eggs, and follicular casts without breaking the skin.
It’s particularly effective for facial and periocular regions and avoids trauma—ideal for sensitive patients or repeated monitoring.
Expressing Follicular Contents
Digital compression of oily areas (like the nasal folds) forces out sebum and cellular debris containing mites. Use a comedone extractor or gloved fingers to express material, then transfer it to a slide with fluorescein.
This method targets both D. folliculorum and D. brevis, though deeper-dwelling D. brevis may require more forceful expression.
When to Use Punch Biopsy
In persistent or atypical cases, a 3–4 mm punch biopsy allows histological evaluation. Stained sections (e.g., H&E) reveal mites within follicular canals and sebaceous glands, confirming infestation even if surface methods fail.
Biopsy is reserved for suspected demodicosis or when differential diagnosis includes other dermatoses.
Visual Features of Demodex Mites

Translucent, Worm-Like Body Shape
Under the microscope, Demodex appears slender and elongated, resembling tiny worms. The body tapers toward the tail, especially in D. folliculorum. Its translucent cuticle reflects little light, making contrast enhancement crucial.
At X100, the segmented trunk and jointed legs are clearly distinguishable. Movement—slow, wriggling motion—confirms the mite is alive and active.
Four Pairs of Short, Stubby Legs
One of the most definitive features is the presence of eight short, segmented legs clustered near the anterior (head) end. These are not used for walking but for anchoring within the follicle.
The legs appear as small protrusions and are best seen under oil immersion. Misidentification with hair fragments or keratin scales can occur if leg segments aren’t clearly visible.
Head-Down Orientation in Follicles
Mites typically reside head-first into the follicle, with the tail end near the skin surface. This orientation is visible in expressed contents and biopsy sections.
Their mouthparts are adapted for scraping skin cells (D. folliculorum) or consuming sebum (D. brevis), reflecting their feeding ecology.
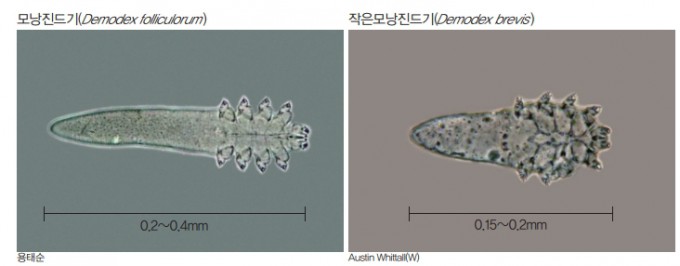
Size Differences Between Species
| Species | Average Length | Appearance |
|---|---|---|
| D. folliculorum | 0.3–0.4 mm | Longer, more slender |
| D. brevis | 0.15–0.2 mm | Shorter, stouter |
Size and shape help differentiate the two species under high magnification. D. brevis’s compact form suits its deeper habitat in sebaceous glands.
Distinguishing Demodex folliculorum vs. brevis
Habitat Depth Determines Detection Method
D. folliculorum lives in the upper infundibulum of the hair follicle, making it easier to collect via surface scraping or tape biopsy. D. brevis, however, resides deep within sebaceous glands, often requiring expression or biopsy for detection.
Because of this, D. brevis is frequently underestimated in routine microscopy unless deeper sampling is performed.
Feeding Habits Linked to Location
- D. folliculorum feeds on keratinocytes (skin cells) and may contribute to follicular blockage.
- D. brevis consumes sebum (lipid secretions), thriving in oily areas like the face and scalp.
These behaviors correlate with clinical findings: high sebum production increases risk for both mite proliferation and associated conditions like sebaceous hyperplasia.
Morphological Clues Under Microscope
While both species share a similar basic structure, subtle differences aid identification:
- D. folliculorum: Longer body, more pronounced tapering at the tail.
- D. brevis: Stockier build, shorter legs relative to body size, adapted for anchoring in glandular ducts.
Only trained observers can reliably distinguish them based on proportions and context.
Common Microscopic Pitfalls and Errors
Mistaking Debris for Mites
Keratin fragments, hair shafts, and dried sebum can mimic Demodex under low magnification. False positives occur when leg segments or head-thorax fusion aren’t clearly visible.
Pro tip: Look for symmetry and jointed limbs. True mites have four pairs of legs; debris rarely mimics this precisely.
Missing Mites Due to Poor Technique
Using dry slides without contrast agents (like fluorescein) reduces visibility. Delayed examination may result in degraded or immobile specimens, making motility—a key sign of viability—impossible to assess.
Always prepare fresh samples and examine promptly.
Relying Solely on Surface Methods
Tape or scraping alone may miss D. brevis due to its deep residence. If clinical suspicion remains high despite negative surface tests, express follicular contents or consider biopsy.
Clinical Correlations Seen Under Microscope
Link to Sebaceous Hyperplasia
Microscopic exams often show abundant D. brevis in specimens with enlarged sebaceous glands. The increased sebum output provides ideal nutrition for mites, creating a feedback loop.
Though causality isn’t proven, the frequent coexistence suggests an ecological relationship worth monitoring in oily or aging skin.
Rosacea and Elevated Mite Counts
Patients with papulopustular rosacea frequently exhibit higher Demodex density per follicle compared to healthy controls. Microscopy reveals multiple mites within a single follicle—sometimes more than five.
Proposed mechanisms include:
– Immune reaction to mite antigens (e.g., chitin, bacterial endosymbionts).
– Follicular blockage from mite accumulation.
– Inflammatory mediators released during feeding.
While Demodex isn’t the sole cause, it acts as a trigger or exacerbating factor in susceptible individuals.
Diagnosing Demodicosis
Demodicosis is confirmed microscopically when:
– More than 5 mites per cm² are found.
– Or ≥6 mites per 6 mm biopsy are observed.
Symptoms include redness, scaling, itching, and follicular plugging—often misdiagnosed as acne or eczema.
Risk factors include:
– Immunosuppression
– Advanced age
– Oily skin
– Long-term steroid use
Microscopy is the gold standard for differentiating demodicosis from mimickers.
Immune Response and Inflammation Clues
Perifollicular Lymphocytic Infiltration
In symptomatic cases, immunohistochemistry shows immune cells clustering around infested follicles. This perifollicular lymphocytic cuffing indicates a type IV hypersensitivity reaction to mite components.
Even without systemic spread, local inflammation can drive chronic redness and papule formation—common in rosacea.
Role of Bacterial Endosymbionts
Bacillus oleronius, found in Demodex gut and feces, may act as an antigen. Immune responses to these bacteria have been linked to IgE activation and cytokine release (e.g., IL-1β, TNF-α), fueling skin inflammation.
Microscopy combined with staining helps correlate mite presence with inflammatory markers.
Expert Tips for Accurate Identification
Train Your Eye to Spot Live Movement
Watch for slow, serpentine motion in fresh samples. Live mites wiggle gently, confirming viability and active infestation. Dead or fixed mites appear rigid and motionless.
This dynamic observation is only possible with immediate examination.
Use Consistent Observer Protocols
Studies show that having one trained observer perform all evaluations reduces variability. Clinicians should standardize their method—same magnification, same contrast agent, same sampling site—to improve accuracy.
Combine Methods for Higher Yield
No single technique detects all mites. For best results:
– Start with tape biopsy or scraping.
– Add expression for deeper mites.
– Reserve biopsy for unclear or resistant cases.
Combining approaches increases detection rates, especially for D. brevis.
Prevention and Management Insights
Reduce Sebum to Limit Habitat
Since both Demodex species rely on sebum and follicular debris, managing oil production helps control populations. Use:
– Gentle cleansers
– Non-comedogenic moisturizers
– Topical agents like metronidazole or ivermectin (prescription)
Tea tree oil (5–50%) has shown efficacy in reducing mite counts due to terpinen-4-ol, a natural acaricide.
Maintain Skin Barrier Integrity
A compromised barrier increases susceptibility. Avoid harsh scrubs, over-washing, or steroid creams unless medically supervised.
Support microbiome balance with prebiotic skincare and minimal disruption.
Monitor High-Risk Patients
Older adults, immunocompromised individuals, and those with rosacea should be periodically assessed. Regular microscopic checks can catch overgrowth before symptoms flare.
Final Note
Viewing Demodex under the microscope reveals a hidden world living on human skin. With X100 oil immersion and fluorescein contrast, these translucent, worm-like mites come into sharp focus—showing eight stubby legs, a head-down posture, and subtle differences between folliculorum and brevis.
Microscopy isn’t just academic—it’s clinically vital. It confirms diagnoses, differentiates species, and links mite burden to conditions like rosacea and sebaceous hyperplasia. By mastering sample collection, avoiding common pitfalls, and interpreting findings in context, clinicians can unlock the role of Demodex in skin health.
Whether you’re a dermatologist, researcher, or curious learner, understanding what Demodex looks like under the microscope brings clarity to one of the most common—and misunderstood—residents of human skin.